Understanding Endometriosis Surgery: Risks and What UK Patients Should Know
⚡ Quick Answer
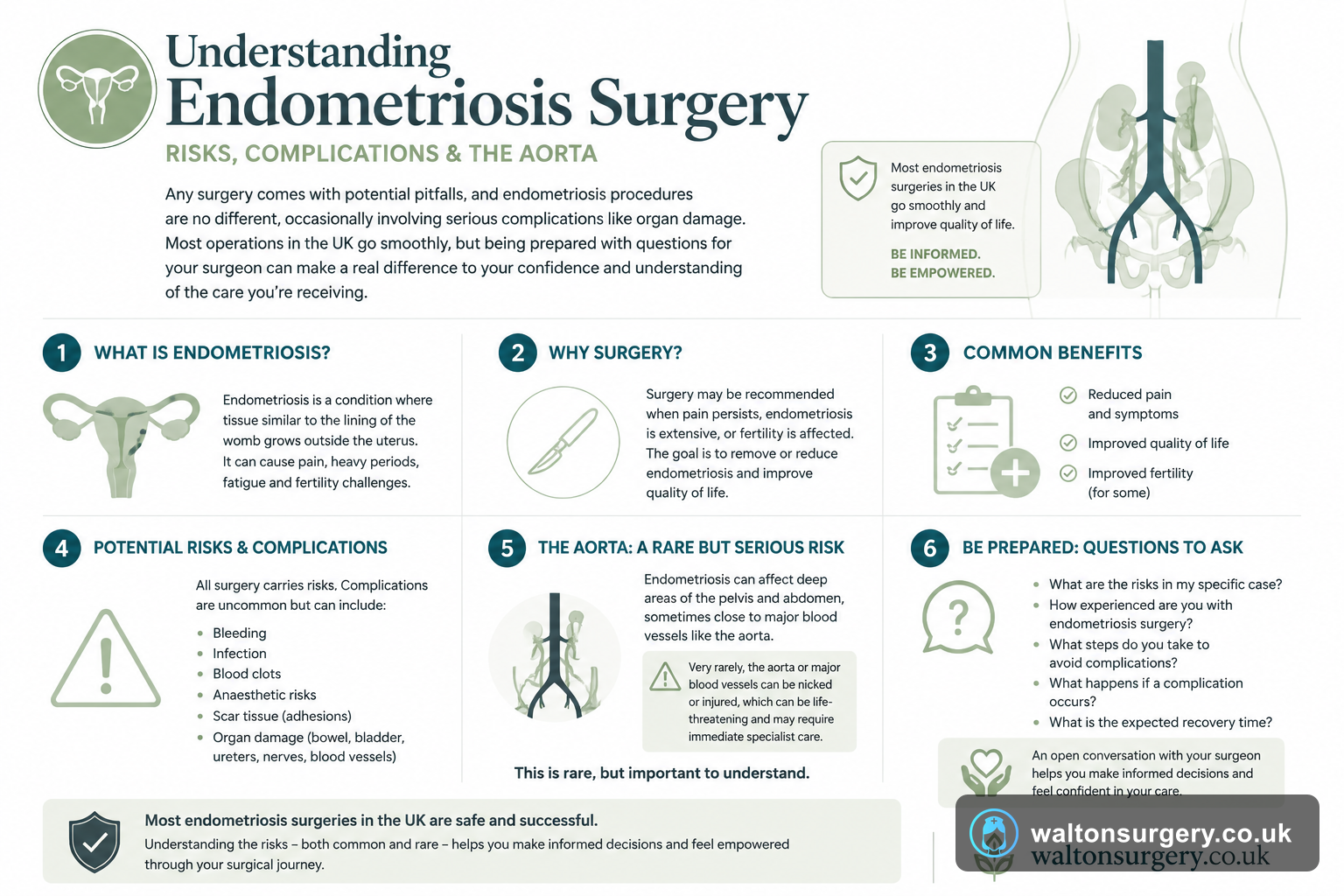
Any surgery comes with potential pitfalls, and endometriosis procedures are no different, occasionally involving serious complications like organ damage. The recent report from actress Leven Rambin regarding an aortic nick serves as a reminder of why you should grasp both frequent and infrequent risks. Most operations in the UK go smoothly, but being prepared with questions for your surgeon can make a real difference to your confidence and understanding of the care you're receiving.
Reading about a famous person suffering a complication during an endometriosis op can be scary, particularly when you are booked in for one yourself. When Leven Rambin shared that her aorta had been accidentally nicked, it naturally made many patients wonder about safety. We're going to break down the real risks associated with this surgery in the UK, using NHS guidance and professional input, so you know what to discuss with your doctors. It is a reminder that surgical risks exist across many procedures, just as discussions around specific conditions like angie best surgery condition often highlight the importance of patient awareness.
What Happened to Leven Rambin and Why Does It Matter to You?
Back in July 2025, the actress went public about an accidental injury to her aorta during her endometriosis procedure. That vessel is the biggest artery we have, and it runs right past the abdominal area where surgeons are usually working. Her story forced a discussion about rare complications that normally stay quiet, causing understandable worry for anyone in the waiting room.
Putting her experience into perspective is useful here. Accidentally damaging a major blood vessel during gynae surgery is actually quite rare. It does occur, though, and being honest about these risks is just standard practice when signing consent forms. This doesn't mean your operation is destined for trouble. What it does suggest is that you are absolutely correct to dig for answers and ensure you feel ready before you sign anything.
How Common Are Complications in Endometriosis Surgery?
Thousands of these operations happen annually across the UK, both via the NHS and in private hospitals. The vast majority occur without a hitch. The NHS acknowledges that every surgical procedure has some degree of risk, and treating endometriosis is certainly included in that.
🔬 Key Facts
Understanding the Odds
- → Minor Issues: Infections and immediate bleeding are the most common problems, handled routinely by staff.
- → Serious Problems: Injuries to the bowel, bladder, ureters, or major blood vessels are recognised but occur much less frequently.
- → Variables Matter: Rates are not static; a simple keyhole removal carries different odds than deep excision involving the bowel.
- → NHS Stance: Updated guidance is clear that patients must be informed that these risks exist prior to consent.
Issues that crop up often are usually on the minor side—things like an infection at the wound site or bleeding that the team deals with straight away. Bladder or bowel troubles that don't last long or bad reactions to the anaesthetic are also on this list. Medical staff handle these quite routinely. Serious problems, however, such as injuries to the bowel, bladder, ureters or major blood vessels, don't happen as much but are still recognised possibilities. The NHS page on consent, which was updated a while back, puts it plainly: you need to know these exist.
Complication rates are not a flat number; they shift depending on how complex the operation is. A simple keyhole removal of surface-level disease is a totally different beast to a deep excision involving the bowel. Your specific case should be the focus of the conversation with your surgeon regarding risk.
Why Is the Aorta at Risk During Pelvic Surgery?
Running down through the abdomen and splitting off into smaller arteries for the pelvic organs, the aorta is always close by. There is a theoretical danger of vascular injury during endometriosis surgery, particularly when the disease has spread widely or is sitting close to those large vessels.
If the endometriosis has burrowed into deep tissue near the blood supply, or if scar tissue (adhesions) has dragged organs into odd places, the risk ticks upward. Surgeons at BSGE-accredited centres deal with this sort of messy anatomy all the time and are specifically trained for it.
The injury Rambin sustained, though infrequent, shows exactly why surgical skill is so vital here. The surgery wasn't reckless; complex endometriosis just puts surgeons in tough spots where even the best hands struggle with the layout. The NHS and the British Society for Gynaecological Endoscopy (BSGE) have pushed hard for specialist centres because of this, rather than having a general gynaecologist attempt the hard stuff.
What Types of Endometriosis Surgery Exist and How Do Their Risks Differ?
Several ways to tackle this surgically exist, and the risks vary for each:
Laparoscopic Excision or Ablation
Laparoscopic excision or ablation happens most often. Small cuts are made, a camera goes in, and the surgeon guides the tools. Risks look like standard keyhole stuff: hernia at the port site, infection, bleeding, or nicking a neighbour. You usually bounce back faster than with open surgery.
Laparotomy (Open Surgery)
Laparotomy, which is open surgery, requires a bigger cut into the abdomen. Doctors use this when the disease is all over the place or they need a direct line of sight. Healing takes longer, and the dangers are those of any big abdominal operation.
Hysterectomy with Excision
Sometimes a hysterectomy with excision is the answer if other methods failed. Taking out the uterus—and occasionally the ovaries—brings its own list of hazards. Removing ovaries means hormonal shifts, on top of the normal major surgery risks. For context on surgical decisions, our recent piece on hannah brown bicorporeal septate uterus surgery uk explainer 2026 covers the specifics of structural uterine interventions. If you want the fuller picture, our guide to almond eye surgery uk cost recovery canthoplasty 2026 explainer goes further.
Deep Endometriosis Excision
Deep endometriosis excision is the hardest version. If the bowel, bladder, or ureters are involved, the surgeon might have to cut out bits of those organs. Leak rates, ureter damage, and needing a temporary stoma are higher here. Both the NHS and BSGE say these must be done in specialist centres with a team of different experts.
Your doctor must be clear about which method is planned and the specific dangers for you. If they aren't, you need to ask.
What Should You Ask Your Surgeon Before Endometriosis Surgery?
You are fully within your rights to ask detailed questions before giving the go-ahead. Consider these:
How many of these have you actually done? Experience is the most reliable sign of a good result. The BSGE thinks complex surgery should only be done by those with a high volume of cases.
Is this hospital a BSGE-recognised specialist centre? They have strict rules on staffing, multi-disciplinary input, and how many surgeries they do.
What are the specific risks in *my* case? Scans showing disease near the bowel or blood vessels change the risk profile drastically compared to superficial issues.
What is the protocol if something goes sideways? Knowing if colorectal surgeons, urologists, or vascular experts are on standby is a sensible thing to check.
What is the aftercare plan? Recovery matters just as much as the knife work.
Don't be shy about asking. A good surgeon appreciates a patient who is clued up. If they brush you off or rush the consent chat, treat that as a major red flag.
What Does the NHS Consent Process Actually Involve?
The NHS demands that patients give informed consent prior to any procedure. You ought to be told what the operation entails, the pros and cons, and what alternatives are available. They also need to tell you what happens if you choose to do nothing and how that might affect your health.
Signing a form is not the whole story. It is a conversation. You should feel like you've had time to think, ask questions, and chat about it with family or friends if you want to. You can pull out of the consent right up until the moment the surgery starts.
If the process felt too fast or incomplete, you can demand another appointment to sort out your worries. The NHS Constitution protects your right to be fully involved in decisions about your own body.
What About Recovery and Complications After Surgery?
How long recovery takes depends on the surgery you had. A straightforward laparoscopy usually lets people get back to normal life in two to four weeks. If it was more complex or an open procedure, you might be looking at six to twelve weeks, or even longer.
Problems can also pop up once you're home. Keep an eye out for:
- Fever or chills, which often point to an infection.
- Abdominal pain that gets worse instead of better.
- Heavy bleeding or discharge that seems odd.
- Trouble going for a pee or a poo.
- Redness, swelling, or discharge from the incision sites.
The NHS says you should contact your surgical team or GP if you notice any of these after leaving the hospital. For a real emergency, dial 999 or head straight to A&E.
Frequently Asked Questions
⭐ The Bottom Line
What this means for you
Endometriosis surgery, like all ops, has its dangers—mostly minor and fixable, but some are serious and rare. What happened to Leven Rambin shows exactly why being informed, asking questions, and ensuring the right person is doing the job in the right place is so vital. You deserve a clear consent process, a surgeon with the right experience, and a solid aftercare plan. If something isn't clear, keep asking until it is.
Last updated: 2026-07-15 · Written by the Walton Surgery editorial team · Medical information is for educational purposes only and does not replace advice from a qualified healthcare professional.