Endometriosis: Symptoms, Causes and How It Is Treated
⚡ Quick Answer
Endometriosis is a long-term condition where tissue similar to the womb lining grows elsewhere in the body. At least 26 celebrities have spoken publicly about living with it. Symptoms include severe period pain, heavy bleeding, and fatigue. Treatments range from hormonal contraception and pain relief to surgery. Seeing your GP is the first step if you suspect you have endometriosis. We cover this in more depth in is it bad to sleep with a fan on overnight uk nhs.
Roughly one in ten women of reproductive age in the UK live with endometriosis. It happens when tissue much like the uterine lining starts growing in places it shouldn't — the ovaries, the fallopian tubes, the pelvic cavity. That misplaced tissue reacts to your hormones just like the real lining would, except it's got nowhere to go. The result is inflammation, chronic pain, and sometimes trouble conceiving.
Names like Lena Dunham, Halsey, and Daisy Ridley have put a public face on the condition in recent years. But fame doesn't speed up the diagnosis process, and plenty of women spend years not knowing what's wrong. So here's what the NHS and other trusted medical bodies actually say about endometriosis — what causes it, how it's diagnosed, what treatments are available, and how people cope with it day to day.
What Exactly Is Endometriosis?
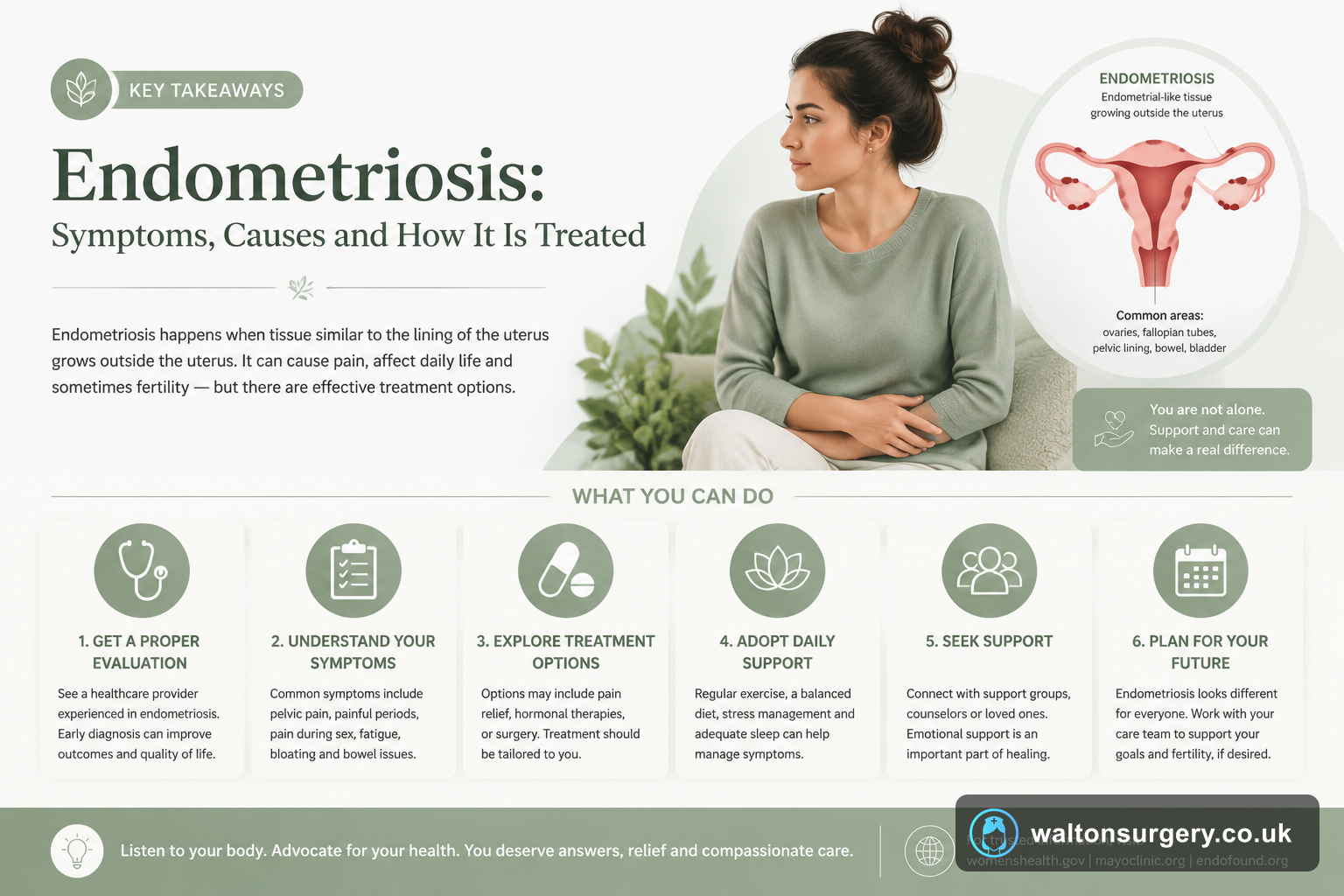
Put simply, endometriosis is tissue that acts like the womb lining but grows outside the uterus. Every month, this tissue responds to your hormonal cycle — it thickens, then breaks down, then bleeds. The problem is, it's stuck inside your body with no exit route. It pools, triggers inflammation, and over time can create scar tissue known as adhesions.
Ovaries, fallopian tubes, and the pelvic lining are the usual spots. Less often it shows up on the bowel, bladder, or even the diaphragm, which is rarer still. What catches people off guard is that the amount of tissue present doesn't predict how much pain you'll feel. Someone with minimal endometriosis can be in agony, while another person with extensive growths might barely notice. We cover this in more depth in best gifts for someone with cancer.
The NHS uses a four-stage classification — minimal, mild, moderate, and severe. These stages describe the location, depth, and volume of the tissue. They don't map neatly onto pain levels.
Symptoms You Should Know About
Pain tops the list, but it's not just bad cramps. According to the NHS, the main symptoms include:
- Periods so painful they stop you doing normal things
- Pain during or after sex
- Discomfort when weeing or opening your bowels during a period
- Heavy bleeding, sometimes with clots
- Struggling to get pregnant
- Ongoing fatigue
- Ache in the lower back, abdomen, or pelvis outside of your period
The variation between people is enormous. Some describe a pain worse than anything they've ever felt before. Others have almost nothing and only find out about the condition when they start investigating fertility problems.
It's also very easy for the symptoms to get mixed up with irritable bowel syndrome, pelvic inflammatory disease, or just "heavy, painful periods" — something you're supposed to put up with. That confusion is a big part of why diagnosis takes so long. The NHS itself acknowledges the average wait from first GP visit to confirmed diagnosis sits at around 7 to 8 years.
Why Does It Happen?
Honestly, nobody knows the exact cause yet. The NHS points to several theories that researchers continue to investigate:
- Retrograde menstruation: menstrual blood flows backwards through the fallopian tubes into the pelvis. Endometrial cells drop out and start growing. The idea has been around for decades, though it doesn't account for every case — plenty of people have retrograde menstruation without ever developing endometriosis.
- Genetic predisposition: it runs in families. If your mum or sister has it, your own risk goes up.
- Immune system problems: the body may fail to recognise and clear out endometrial tissue that's growing where it shouldn't.
- Metaplasia: existing cells in the pelvic area transform into endometrial-type cells. It's a theory that's harder to test.
None of these explanations covers all cases, which is partly why funding and research are still so important. What clinicians are fairly certain about is that endometriosis isn't something you caused through behaviour. It isn't an infection. It's not sexually transmitted.
How Is Endometriosis Diagnosed?
Your GP will usually start with a conversation about your symptoms and might do an internal examination. Blood tests and ultrasound scans can be useful, though they don't always pick endometriosis up.
The definitive test is a laparoscopy — keyhole surgery under general anaesthetic. A surgeon makes a small cut near your belly button, inserts a tiny camera, and looks around the pelvic area. If they spot endometriosis tissue, they can take a biopsy to send off for testing. Understanding the potential endometriosis surgery risks complications aorta is an important part of preparing for this procedure.
Some hospitals have started using MRI scans to help, particularly when they suspect deep endometriosis affecting the bowel or bladder. But as things stand, laparoscopy remains the gold standard for a clear diagnosis.
Lena Dunham and Halsey have both talked openly about the frustration of multiple doctor visits before anyone gave them a straight answer. If you feel your symptoms are being dismissed, pushing for a referral to a gynaecologist is absolutely within your rights.
Treatment Options Available Through Your GP and Specialist
There's no cure for endometriosis at the moment. That said, there are treatments that genuinely help manage symptoms and improve day-to-day life. The approach depends on how severe things are, whether you want children in future, and how much the condition is affecting you.
Pain relief
Over-the-counter options like ibuprofen and paracetamol are usually the first recommendation. When those don't cut it, a GP can look at stronger prescriptions.
Hormonal treatments
Reducing or stopping periods often eases endometriosis symptoms significantly. Hormonal contraception options include:
- The combined pill, taken back-to-back without the usual break
- The progestogen-only pill
- The contraceptive injection or implant
- The intrauterine system (IUS) — Mirena is the one most people have heard of
- GnRH analogues, which put the body into a temporary menopause-like state and are used under specialist guidance
Surgery
When hormonal treatments aren't enough, or when the endometriosis is moderate to severe, surgery becomes an option. A laparoscopy can remove or destroy tissue using heat (diathermy) or laser. In serious cases — after other options have been tried — removal of affected organs might be discussed, including a hysterectomy. It's a major operation and a decision that takes real thought.
Hertility Health and the Royal College of Obstetricians and Gynaecologists (RCOG) both emphasise the importance of personalised treatment. What works brilliantly for one woman may do very little for another.
What About Fertility?
Not everyone with endometriosis will struggle to get pregnant, but the condition can make it harder. The NHS puts the figure at roughly 30-50% of women with endometriosis experiencing difficulty conceiving. If starting a family is on your mind, it is worth having that conversation with your GP sooner rather than later. Options range from surgery to clear endometriosis tissue through to assisted conception techniques like IVF.
🔬 Key Facts
Diagnosis and Symptoms
- → Average wait time for diagnosis in the UK is 7 to 8 years from first GP visit.
- → Laparoscopy is the gold standard for a definitive diagnosis.
- → Symptoms often overlap with IBS, fibroids, and pelvic inflammatory disease.
Living With Endometriosis: Managing Day to Day
Medical treatment is one piece of the puzzle. The NHS and Endometriosis UK recommend practical steps that can make real day-to-day differences:
- Heat therapy: a hot water bottle or heat pad pressed against your lower abdomen can take the edge off pain.
- Gentle exercise: walking, swimming, yoga — anything that keeps you moving without overdoing it. The ISSN (International Society of Sports Nutrition) hasn't published endometriosis-specific research, but general guidance on chronic pain supports low-to-moderate activity.
- Diet: cutting back on caffeine, alcohol, or highly processed food seems to help some women, although no large-scale clinical trials back a particular endometriosis diet.
- Support: Endometriosis UK runs support groups across the country and operates a helpline. Speaking to people who actually understand what you're going through can matter more than you'd think.
- Workplace adjustments: if the condition affects your capacity to work, the Equality Act 2010 gives you a right to reasonable adjustments. Endometriosis can qualify as a disability when it substantially limits everyday activities.
Celebrities including Whoopi Goldberg and Padma Lakshmi have spoken publicly about the impact on their careers and routines. That visibility helps chip away at the isolation many women feel.
Why Diagnosis Takes So Long — And What You Can Do About It
Seven to eight years — that's the UK average from first GP visit to confirmed diagnosis, according to Endometriosis UK and NHS data. Several things feed into that delay:
- The symptoms overlap with IBS, fibroids, and pelvic inflammatory disease.
- Period pain is routinely normalised — by society and, occasionally, by clinicians.
- A definitive diagnosis requires a surgical referral for laparoscopy, which takes time.
So what can you actually do? Keep a symptom diary. Write down when the pain hits, how bad it gets, and how it affects your day. Bring it along to your appointment. If you feel brushed aside, ask for a second opinion or specifically request a referral to a gynaecologist experienced in endometriosis.
Frequently Asked Questions
⭐ The Bottom Line
What this means for you
Endometriosis is common yet still poorly understood by many. High-profile women sharing their stories have moved the conversation forward, but the average person still waits the better part of a decade for answers. If what you've read here rings true for your own experience, book that GP appointment and be honest about what you're dealing with. Treatments that actually work do exist, and getting proper support can transform how you live with this condition.
Last updated: 2026-07-15 · Written by the Walton Surgery editorial team · Medical information is for educational purposes only and does not replace advice from a qualified healthcare professional.